9.20. Whooping Cough (Pertussis)
Guidelines for Managing Whooping Cough (Pertussis)
This guidance is intended to assist healthcare workers in the management of patients, staff, and visitors who present with symptoms suggestive of whooping cough. These guidelines should be implemented to prevent and control the spread of infectious diseases and to help avert outbreaks.
Overview
Whooping cough, also known as pertussis, is a highly contagious bacterial respiratory infection caused by Bordetella pertussis. It is characterized by severe coughing spells that can end with a “whooping” sound when the person breathes in. It is particularly dangerous for infants, young children, and vulnerable populations.
Mode of Transmission
| Route | Description |
|---|---|
| Primary route | Airborne transmission through respiratory droplets when an infected person coughs, sneezes, or talks. |
| Close contact | Direct contact with discharges from respiratory mucous membranes of an infected person, or contact with surfaces contaminated with respiratory secretions. |
The disease is frequently brought home by an older sibling or a parent.
Incubation Period
The incubation period typically ranges from 7 to 10 days but can extend up to 21 days.
Period of Communicability (Infectious Period)
- Whooping cough is highly communicable from the onset of catarrhal symptoms before the paroxysmal cough stage.
- Communicability gradually decreases and is negligible after 3 weeks for ordinary non-familial contacts, despite persisting spasmodic cough with whoop.
Susceptibility and Resistance
- There is no clear evidence of effective trans-placental immunity in infants.
- It is predominantly a childhood disease, with incidence rates highest in the under-5 age group.
- One attack usually confers prolonged immunity, although second attacks can occur occasionally.
- Cases in adolescents and adults occur because of incomplete immunizations and waning immunity.
Clinical Signs and Symptoms
Whooping cough progresses through three stages:
| Stage | Typical Duration | Key Features |
|---|---|---|
| Catarrhal stage | 1–2 weeks | Mild, cold-like symptoms, including runny nose, sneezing, low-grade fever, and mild cough. The patient is highly contagious during this stage. |
| Paroxysmal stage | 1–6 weeks | Severe coughing fits, known as paroxysms, followed by a “whooping” sound during inhalation. Vomiting or exhaustion may occur after coughing spells. |
| Convalescent stage | Weeks to months | Gradual reduction in coughing frequency and severity. Cough may persist for weeks or months. |
Complications
Infants and Young Children
- Pneumonia
- Seizures
- Encephalopathy
- Apnea
- Death
Adolescents and Adults
- Weight loss
- Rib fractures
- Urinary incontinence
- Syncope due to severe coughing
Diagnosis
Clinical Evaluation
Diagnosis is based on symptoms, especially the characteristic “whoop” and prolonged cough.
Laboratory Tests
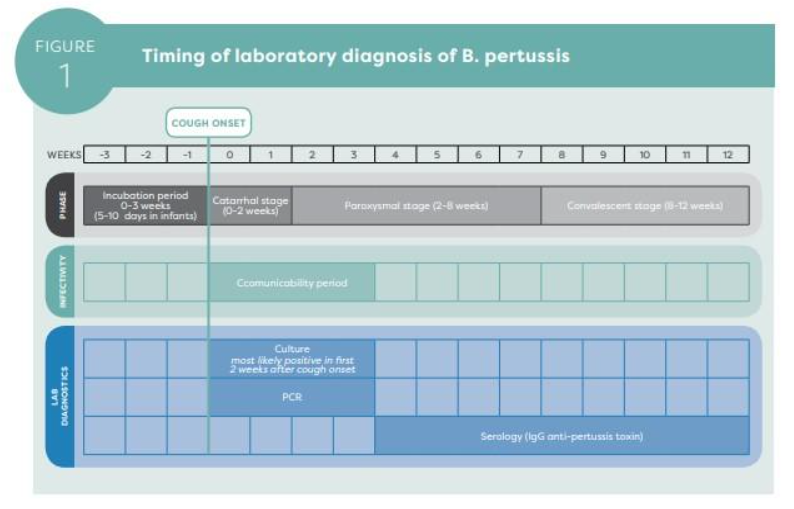
Please complete the Ezra Long Communicable Disease Laboratory Requisition Form requesting testing for Bordetella pertussis when taking a nasopharyngeal swab on a suspected case.
Serology may be used to detect antibodies, particularly in later stages of illness, from 4–12 weeks after cough onset.
Specimen Collection
| Time from Cough Onset | Recommended Specimen | Key Instructions |
|---|---|---|
| Within 4 weeks | Nasopharyngeal swabs for culture and PCR |
|
| 4–12 weeks | Serum sample for IgG anti-pertussis toxin antibody testing |
|
Case Definitions
Suspected Case
A person of any age with a cough lasting 2 weeks or longer, or of any duration in an infant or any person in an outbreak setting, without a more likely diagnosis and with at least one of the following:
- Paroxysms or fits of coughing
- Inspiratory whooping
- Post-tussive vomiting, or vomiting without other apparent cause
- Apnea, only in infants younger than 1 year of age
- Clinician suspicion of pertussis
Confirmed Case
A confirmed case may be determined by laboratory confirmation or epidemiological linkage.
Laboratory-confirmed Case
A person who meets the suspected case definition with laboratory confirmation by either of the following:
- Detection of genomic sequences of B. pertussis by PCR assay meeting performance criteria; or
- Elevated IgG antibodies to pertussis toxin in an individual 11 years of age or older, one year or longer after the last vaccine dose.
Epidemiologically Linked Case
A person meeting the suspected case definition with close contact to a laboratory-confirmed case, or another epidemiologically linked case in an outbreak setting, in the three weeks prior to onset of cough.
Possible Case
A person who meets the suspected case definition but does not meet confirmed classification. This includes suspected cases who did not have laboratory testing done and those who tested negative.
Prevention and Control
Vaccination
- Current vaccination coverage in Saint Lucia is 89% as of 2024.
- Ideal coverage is 95% and above.
- Continued advocacy for vaccination is essential.
- Pregnant women should receive DT during each pregnancy, preferably between 27–36 weeks gestation, to protect newborns through passive antibody transfer.
- DPT is given from 2 months to 5 years.
Isolation and Quarantine
Exposed household members and close contacts should receive prophylactic antibiotics.
Antibiotic Prophylaxis
Management of Contacts
Definition of a Close Contact
A close contact is a person with face-to-face exposure, within 1 metre, to an infectious case for a single period of at least one hour. This also includes family and household members and, in other settings, people who have stayed overnight in the same room as the case.
Asymptomatic Close Contacts
Asymptomatic close contacts are not contagious and do not need to be excluded from social settings. They should be monitored for the development of symptoms for 21 days following last exposure.
Symptomatic Contacts
- If symptomatic contacts have already coughed for 21 days at the time of diagnosis, the individual is no longer contagious and isolation is not indicated.
- Symptomatic contacts who refuse antibiotics should stay home, excluding school, child care, work, church, and other social settings, for 21 days after cough onset. During this period, they should not receive visitors.
Key Messages for Healthcare Workers
- Maintain a high index of suspicion for whooping cough, especially in infants and unvaccinated individuals, particularly those residing in communities where an infected case has stayed.
- Ensure nasopharyngeal swab specimen collection from any suspected case of whooping cough.
- Immediately notify any suspected cases to the Epidemiology Unit at the Ministry of Health.
- Advocate for vaccination as the most effective preventive measure for unvaccinated persons.
- Use azithromycin as first-line antibiotic for treatment and prophylaxis unless contraindicated.
Reference List
- World Health Organization. (2023). Surveillance Vaccine Preventable Diseases: Pertussis. Available from: https://cdn.who.int/media/docs/default-source/immunization/vpd_surveillance/vpd-surveillance-standards-publication/who-surveillancevaccinepreventable-16-pertussis-r2.pdf
- Centers for Disease Control and Prevention. (2024). Pertussis (Whooping Cough): Clinical Features. Available from: https://www.cdc.gov/pertussis/clinical/index.html
- Pan American Health Organization / World Health Organization. (2024). Pertussis: Epidemiological Alerts and Updates.